Hyperpigmentation is uneven and excessive skin pigmentation presenting as localised areas of darker skin tone, commonly affecting the face, hands, and other sun-exposed areas. Causes range from UV exposure, genetics, natural ageing and hormonal fluctuations to skin trauma, medication, heat, and visible and infrared light. The most common forms of hyperpigmentation include freckles, sunspots, post-injury pigmentation called post-inflammatory hyperpigmentation, and melasma.


Doctor’s certificate for a skin cancer check must be provided prior to pigmentation treatments.

Small flat pigmented spots on the face, arms, and other sun-exposed areas, less visible in winter and darker with sun exposure.
Causes: UV radiation and genetics

Flat brown age spots larger than freckles, common in adults over 40 on the face, hands, and other sun-exposed areas.
Causes: Cumulative UV radiation and natural ageing

Skin darkening at sites of previous injury or inflammation, most commonly from acne, skin picking, burns, and cuts. Typically fades over time but can be prolonged.
Causes: Skin trauma and prolonged skin inflammation

Complex and chronic skin condition causing often symmetrical brown or grey-brown pigmented patches, most commonly on the cheeks, forehead, upper lip, and chin.
Causes: UV radiation, hormonal fluctuations, genetics, and visible and infrared light.
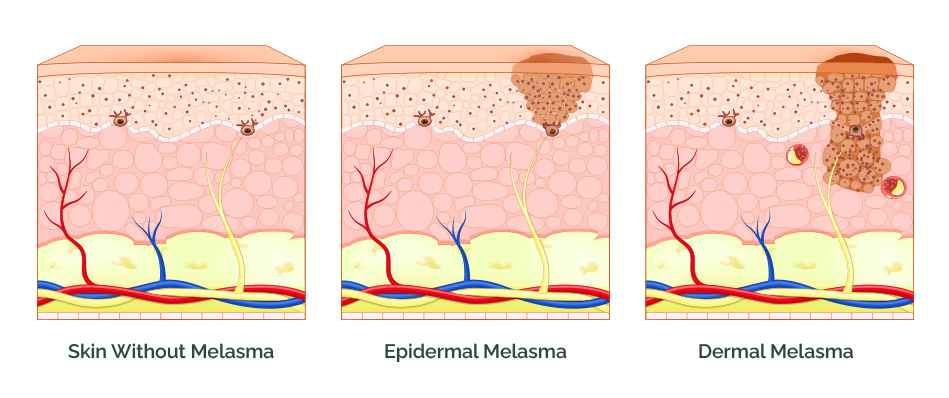
Melasma occurs in three forms depending on the depth of pigment within the skin – epidermal melasma, where excess melanin is confined to the upper skin layers and typically appears as well-defined brown patches; dermal melasma, where pigment is deposited deeper within the dermis and presents as less defined, grey-brown patches; and mixed melasma, the most common form, involving both epidermal and dermal pigment deposition. The depth of melasma directly influences how it responds to treatment – epidermal melasma generally responds better and faster, while dermal and mixed melasma require more treatments and a carefully tailored approach to achieve results and minimise the risk of pigment relapse.





| INGREDIENT & ACTION | Inhibits Melanin Production | Blocks Melanin Transfer | Increases Cell Turnover | Antioxidant Protection | Reduces Skin Inflammation | Strengthens Skin Barrier |
|---|---|---|---|---|---|---|
| Retinoids (Retinol, Retinal, Retinoic Acid)* | ++ | ++ | +++ | + | ++ | + |
| Niacinamide | ++ | +++ | + | ++ | +++ | +++ |
| L-Ascorbic Acid (Vitamin C) | +++ | – | – | +++ | ++ | – |
| Tranexamic Acid | ++ | – | – | + | +++ | – |
| Resorcinol Derivatives (Hexylresorcinol & 4-Butylresorcinol) | +++ | – | – | + | ++ | – |
| Lactic & Mandelic Acid (AHAs) | + | – | +++ | ++ | + | ++ |
| Kojic Acid | +++ | – | – | + | + | – |
| Hydroquinone** (prescription) | +++ | – | – | – | – | – |
| Grading: +++ Strong action ++ Moderate action + Mild action – Not applicable *Topical retinoids range in strength and delivery system — retinoic acid, a prescription retinoid, delivers faster results but carries a higher irritation potential. **Hydroquinone is prescription-only in Australia and other countries and long-term use carries risks of pigment relapse. |
| INGREDIENT & ACTION | Inhibits Melanin Production | Blocks Melanin Transfer | Increases Cell Turnover | Antioxidant Protection | Reduces Skin Inflammation | Strengthens Skin Barrier |
|---|---|---|---|---|---|---|
| Glabridin (from Liquorice Root Extract) | +++ | – | – | +++ | +++ | – |
| Resveratrol | ++ | – | – | +++ | +++ | – |
| Silymarin (Milk Thistle) | ++ | – | – | +++ | ++ | – |
| Bakuchiol | ++ | ++ | +++ | +++ | ++ | ++ |
| Gluconolactone & Lactobionic Acid (PHAs) | – | – | ++ | +++ | + | ++ |
| Alpha-Arbutin | +++ | – | – | + | – | – |
| Cysteamine | +++ | – | – | +++ | + | – |
| Grading: +++ Strong action ++ Moderate action + Mild action – Not applicable |




